PREVIOUS
✖
Litchi toxin and deaths of children
June 29 , 2019
2113 days
3041
0
- Acute encephalitis syndrome (AES) in Bihar’s Muzaffarpur, Vaishali, Sheohar and East Champaran districts has so far claimed the lives of over 100 children.
- More than 400 children with AES have been admitted to various hospitals.
- Most of the deaths have been attributed to low blood sugar level (hypoglycemia).
What is acute encephalitis syndrome?
- AES in short, it is a basket term used for referring to hospital, children with clinical neurological manifestations which include mental confusion, disorientation, convulsion, delirium or coma.
- Meningitis caused by virus or bacteria, encephalitis (mostly Japanese encephalitis) caused by virus, encephalopathy, cerebral malaria, and scrub typhus caused by bacteria are collectively called acute encephalitis syndrome.
- While microbes cause all the other conditions, encephalopathy is biochemical in origin, and hence very different from the rest.
- There are different types of encephalopathy.
- In the present case, the encephalopathy is associated with hypoglycaemia and hence called hypoglycaemic encephalopathy.
Is encephalitis different from hypoglycaemic encephalopathy?
- The two conditions show very different symptoms and clinical manifestations.
- Fever on the first day is one of the symptoms of encephalitis before the brain dysfunction begins.
- While fever is seen in children in the case of hypoglycaemic encephalopathy, fever is always after the onset of brain dysfunction (actually due to the brain dysfunction). And not all children exhibit fever.
- Some children have no fever, while others may have mild or very high fever.
- The blood sugar level is usually normal in children with encephalitis but is low in children with hypoglycaemic encephalopathy.
- In the case of encephalitis, fever (due to virus infection) for a day or two is followed by the onset of symptoms caused by the brain getting affected.
- However, in hypoglycaemic encephalopathy, children go to bed without any illness but manifest symptoms such as vomiting, convulsion and semi-consciousness early next morning (between 4 a.m. to 7 a.m.).
- At that time, the blood sugar level is low, hence the name hypoglycaemic encephalopathy.
- The most important difference between the two is the presence of white blood cells in the cerebrospinal fluid.
- In encephalitis, there are more white blood cells per unit volume of cerebrospinal fluid, which is a reflection of inflammation in the brain.
- In contrast, no increase in white blood cells is seen in hypoglycaemic encephalopathy as there is no inflammation in the brain.
What killed so many children in Bihar?
- In a majority of cases, children died due to hypoglycaemic encephalopathy.
- According to a Press Information Bureau (PIB) release, hypoglycaemia (low blood sugar level) was reported in a “high percentage” of children who died in Muzaffarpur.
- Unlike hypoglycaemic encephalopathy, encephalitis does not cause low blood sugar level so death in a high percentage of children couldn’t have been due to encephalitis.
Why it affected only young children?
- It is an observed fact that malnourished children between two to 10 years fall ill and die due to hypoglycaemic encephalopathy.
- It is not known why older children or adults do not suffer the same way.
- This clear discrimination by age is also a reason why the underlying cause of the illness cannot be a virus.
- A virus does not discriminate by age, and children younger than two years too are affected by Japanese encephalitis.
- It has also been documented that most of the children falling ill are from families camping in orchards to harvest the fruits.
- These children tend to collect and eat the fruits that have fallen on the ground.
Is litchi fruit responsible for causing hypoglycaemic encephalopathy?
- In 2012-2013, a two-member team headed by virologist Dr. T. Jacob John suspected, and confirmed in the next year that a toxin found in litchi fruit was responsible for causing hypoglycaemic encephalopathy.
- In 2017, an India-U.S. team confirmed the role of the toxin called Methylene Cyclo Propyl Glycine (MCPG).
- Early morning, it is normal for blood sugar to dip after several hours of no food intake.
- Undernourished children who had gone to sleep without a meal at night develop hypoglycaemia.
- The brain needs normal levels of glucose in the blood.
- The liver is unable to supply the need.
- So, the alternate pathway of glucose synthesis, called fatty acid oxidation, is turned on. That pathway is blocked by MCPG.
- Litchi does not cause any harm in well-nourished children, but only in undernourished children who had eaten litchi fruit the previous day and gone to bed on an empty stomach.
Why is the toxin more dangerous for undernourished children?
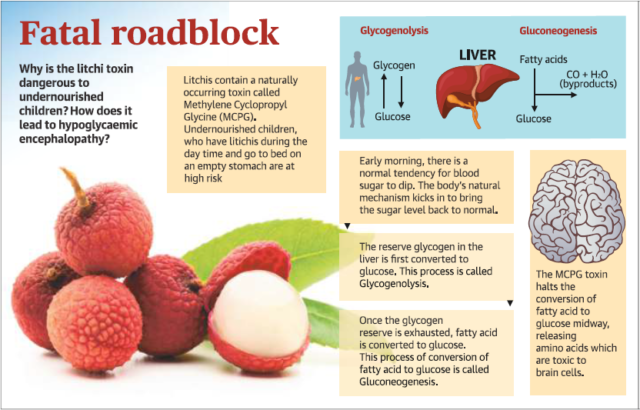
- In well-nourished children, reserve glucose is stored as glycogen (glucose polysaccharide) in the liver.
- Whenever the glucose level goes down, glycogen is broken down into glucose and circulated in the blood for use.
- But undernourished children lack sufficient glycogen reserve that can be converted into glucose.
- Therefore, the natural mechanism in undernourished children is unable to correct the glucose level in blood, leading to hypoglycaemia.
- Normally, when glycogen reserve in the liver is exhausted or is not sufficient, the body converts the fatty acid (non-carbohydrate energy source) into glucose.
- But in the presence of the litchi toxin, the conversion of fatty acid into glucose is stopped midway.
- As a result, no glucose is generated and the low blood glucose level is not corrected by the body.
How do the toxin cause coma and even death in children?
- The toxin acts in two ways to harm the brain and even cause death.
- Because of the toxin, the body’s natural mechanism to correct low blood glucose level is prevented thus leading to a drop-in fuel supply to the brain.
- This leads to drowsiness, disorientation and even unconsciousness.
- When the toxin stops the fatty acid conversion into glucose midway, amino acids are released which are toxic to brain cells.
- The amino acids cause brain cells to swell resulting in brain oedema.
- As a result, children may suffer from convulsions, deepening coma and even death.
Is hypoglycaemic encephalopathy can preventable?
- Yes, by making sure that undernourished children do not eat plenty of litchi fruit, ensuring that they eat some food and not go to bed on an empty stomach.
- In 2017, the India-U.S. team published a paper corroborating these findings and recommendations.
Can hypoglycaemic encephalopathy be treated?
- Yes, hypoglycaemic encephalopathy can be easily treated.
- A full and complete recovery can be achieved if children with hypoglycaemic encephalopathy are infused with 10% dextrose within four hours after the onset of symptoms.
- Infusing 10% dextrose not only restores blood sugar to a safe level but also stops the production of amino acid that is toxic to brain cells by shutting down the body’s attempt to convert fatty acid into glucose.
- Together with dextrose infusion, infusing 3% saline solution helps in reducing oedema of the brain cells.
- The concentration of ions in the fluid outside the brain cells becomes more than what is inside the cell.
- This causes the fluid from the cells to come out thus reducing oedema and damage to brain cells.
- Using 5% dextrose, as is the norm in cases of general low blood sugar level, may help children with hypoglycaemic encephalopathy recover from hypoglycaemia, but the accumulation of amino acid is not turned off.
- And so, even if children survive, they will have brain damage.
- If dextrose infusion is not started within four hours after the onset of symptoms, the brain cells may not recover but will die.
- As a result, even if they survive, children suffer from various aspects of brain damage speech getting affected, mental retardation, muscle stiffness/weakness and so forth.
- - - - - - - - - - - - - - -

Leave a Reply
Your Comment is awaiting moderation.